What is myopia?
“A refractive error in which rays of light entering the eye parallel to the optic axis are brought to a focus in front of the retina when ocular accommodation is relaxed. This usually results from the eyeball being too long from front to back, but can be caused by an overly curved cornea and/or a lens with increased optical power. It also is called nearsightedness.”
Myopia is a common cause of correctable vision loss, with uncorrected myopia remaining the leading cause of distance vision impairment globally. Individual studies show variations in the prevalence of myopia and high myopia across regions and ethnic groups. And recent landmark publication estimates that by 2050, half the world population will have myopia.

Myopia has been the subject of major international research for decades, directed towards understanding the development of this condition and how we can prevent, or slow it down. The number of people affected by myopia is now increasing around the world, and is projected to affect fifty per cent of the world population by 2050,1 due mainly to lifestyle factors.
Myopia has also been shown to increase the risk of sight threatening complications for example, glaucoma,2 cataract3 and retinal detachment.4
An unknown but frequent cause of vision impairment and blindness in East Asia and Europe is myopic macular degeneration.
The WHO held a Global Scientific Meeting on Myopia at the Brien Holden Vision Institute in Sydney, Australia in 2015 to address the public health issue of myopia, the classification of myopia, evidence for treatments, and the need to take action.
Prevalence
Evidence is mounting that myopia is growing around the world, with a recent study estimating that on average, 30% of the world is currently myopic and by 2050, almost 50% will be myopic, that’s a staggering 5 billion people.1 The hot spots of myopia are East and South East Asia where countries such as South Korea,5 Taiwan,6 Singapore,7 China8 and Japan9 have a prevalence of myopia of 80 to 90 %. But myopia prevalence is rising and the USA has reported a prevalence of 42%, almost doubling in three decades.10
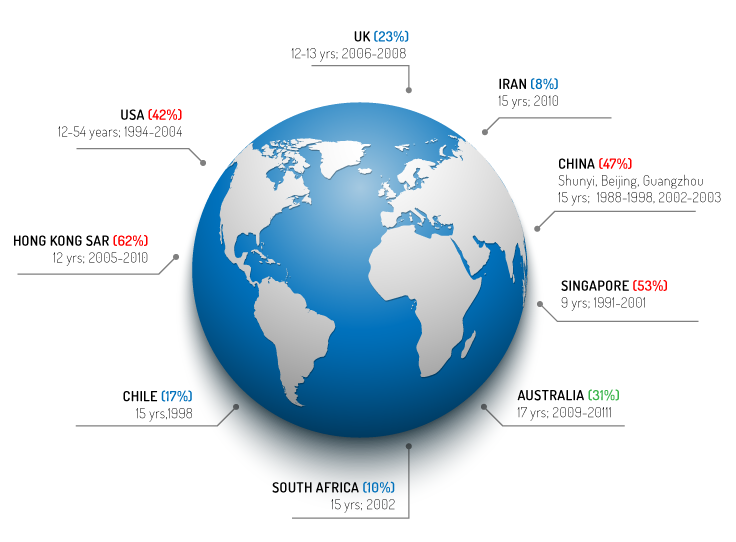
GLOBAL SNAPSHOT
This is a snapshot of the rate of myopia seen in children based on recent studies. (Right). More recent studies indicate that myopic macular degeneration is becoming a serious ocular health issue, where it has been reported one of the major causes of permanent blindness in Rotterdam11, Copenhagen12, China13, Chinese Taipei14, and Japan15.
KEY FINDINGS
- Almost 5 billion myopes by 20501
- Almost 1 billion high myopes by 20501
- Myopia to become a leading cause of permanent blindness worldwide1
- Significant implications for planning comprehensive eye care services globally1
Sources from image stats: McCullough et al. 2016 (UK)18
FUTURE EPIDEMIC
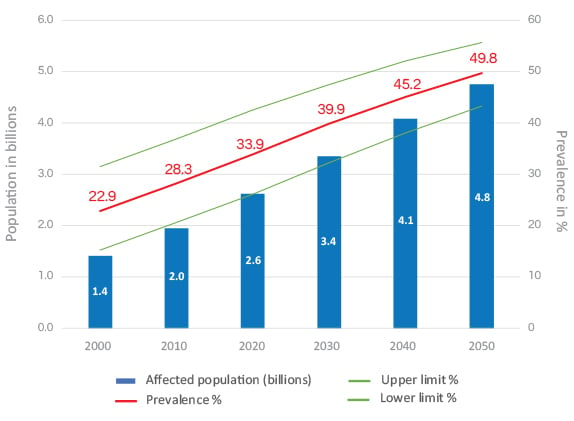
RISING PREVALENCE OF MYOPIA: 2010 TO 2050
The recent Sydney Myopia Study found 31% of 17 year olds were myopic,16 double the prevalence reported by the Blue Mountain Eye Study more than a decade ago.17 But in the future, even nations which have little myopia today, will be severely affected.1 And so good future planning of eye care service and delivery will be required.
Impact
We estimate that myopia and high myopia will show a significant increase in prevalence globally, affecting nearly 5 billion people and 1 billion people, respectively, by 2050. These have important implications for planning comprehensive eye care services, including refractive services such as spectacles and managing and preventing myopic-related ocular complications and vision loss among people with high myopia.
POTENTIAL CONSEQUENCES

Uncorrected refractive error (URE) will increase substantially

Cataract and Glaucoma-Fraction attributable to myopia likely to increase

Blindness and vision impairment due to myopic macular degeneration (MMD) and myopia retinopathy in adults will increase substantially

Resources: Need for refractive and specialist services (spectacles, contact lenses) for managing myopia-related complications will increase
Economic consequences
Global cost of distance ure $202Bn per year in 200920,21 of which myopia is the main cause. The global cost of myopia from lost productivity due to vision impairment from uncorrected myopia and myopic macular degeneration was estimated to be USD 244 billion in 2015.22
| Blindness | 1990 | 2010 |
|---|---|---|
| 1. Cataract | 38.6% | 33.4% |
| 2. Uncorrected Refractive Error | 19.9% | 20.9% |
| 3. Macular Degeneration | 4.9% | 6.6% |
| 4. Glaucoma | 4.4% | 6.6% |
| 5. Diabetic Retinopathy | 2.1% | 2.6% |
| 6. Trachoma | 2.8% | 1.4% |
| 7. Other Causes | 27.4% | 28.6% |
| Moderate to severe vision impairment | 1990 | 2010 |
|---|---|---|
| 1. Uncorrected Refractive Error | 51.1% | 52.9% |
| 2. Cataract | 25.6% | 18.4% |
| 3. Macular Degeneration | 1.9% | 3.1% |
| 4. Glaucoma | 1.2% | 2.2% |
| 5. Diabetic Retinopathy | 1.3% | 1.9% |
| 6. Trachoma | 1.3% | 0.7% |
| 7. Other Causes | 17.6% | 20.8% |
IMPACT ON LEARNING AND EDUCATION
Solution
The International Myopia Institute arose, as an initiative of the late Professor Brien Holden of the Brien Holden Vision Institute, who recognised the need to address the issues surrounding myopia, such as the growing prevalence of myopia around the world, the risks to vision, how clinicians should best manage myopia based on the latest evidence, while further advancing myopia research.
Myopia needed to be recognized as a public health issue if there was to be a change in the approach to this condition, and only a collaborative effort across all eye care professions and researchers could bring this about. Under the auspices of the International Myopia Institute, experts from different myopia-related fields have come together, so that synergistic effects could develop and to make their latest research accessible and easy to understand for practitioners, governments, policy makers, educators, and the general public.
The future initiatives and role of The International Myopia Institute will be to foster these scientific cooperations, to be a platform for further harmonization of definitions and guidelines, and also to promote the connections between the scientific world and the public, ultimately supporting the advocacy of this issue at the level of governments, peak health and regulating bodies.
Membership
The International Myopia Institute is a non-profit global organisation that will bring together all the researchers, clinicians, educators and policy makers, as well as all the information about myopia, making it accessible and easy to understand, and aims to promote the values of scientific integrity, collegiality, evidence based knowledge and preventing future blindness.
Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, Wong TY, Naduvilath TJ, Resnikoff S, Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050, Ophthalmology, May 2016 Volume 123, Issue 5, Pages 1036–1042.
Qiu M, Wang SY, Singh K, Lin SC. Association between myopia and glaucoma in the United States population. Investigative ophthalmology & visual science 2013;54:830-5.
Younan C, Mitchell P, Cumming RG, Rochtchina E, Wang JJ. Myopia and incident cataract and cataract surgery: the blue mountains eye study. Investigative ophthalmology & visual science 2002;43:3625-32.
Group TEDC-CS. Risk factors for idiopathic rhegmatogenous retinal detachment. The Eye Disease Case-Control Study Group. American journal of epidemiology 1993;137:749-57.
Jung SK, Lee JH, Kakizaki H, Jee D. Prevalence of myopia and its association with body stature and educational level in 19-year-old male conscripts in seoul, South Korea. Investigative ophthalmology & visual science 2012;53:5579-83.
Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese schoolchildren: 1983 to 2000. Annals of the Academy of Medicine, Singapore 2004;33:27-33.
Quek TP, Chua CG, Chong CS, et al. Prevalence of refractive errors in teenage high school students in Singapore. Ophthalmic & physiological optics : the journal of the British College of Ophthalmic Opticians 2004;24:47-55.
He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB. Refractive error and visual impairment in urban children in southern china. Investigative ophthalmology & visual science 2004;45:793-9.
Matsumura H, Hirai H. Prevalence of myopia and refractive changes in students from 3 to 17 years of age. Survey of ophthalmology 1999;44 Suppl 1:S109-15.
Vitale S, Sperduto RD, Ferris FL, 3rd. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Archives of ophthalmology 2009;127:1632-9.
Verhoeven VJ, Wong KT, Buitendijk GH, Hofman A, Vingerling JR, Klaver CC. Visual consequences of refractive errors in the general population. Ophthalmology. 2015;122(1):101-9.
Buch H, Vinding T, La Cour M, Appleyard M, Jensen GB, Nielsen NV. Prevalence and causes of visual impairment and blindness among 9980 Scandinavian adults: the Copenhagen City Eye Study. Ophthalmology. 2004;111(1):53-61.
Tang Y, Wang X, Wang J, Huang W, Gao Y, Luo Y, et al. Prevalence and Causes of Visual Impairment in a Chinese Adult Population: The Taizhou Eye Study. Ophthalmology. 2015.
Tsai IL, WoungLC, Tsai CY, Kuo LL, Liu SW, Lin S, et al. Trends in blind and low vision registrations in Taipei City. Eur J Ophthalmol. 2008;18(1):118-24.
Iwase A, Araie M, Tomidokoro A, Yamamoto T, Shimizu H, Kitazawa Y, et al. Prevalence and causes of low vision and blindness in a Japanese adult population: the Tajimi Study. Ophthalmology. 2006;113(8):1354-62.
Attebo K, Ivers RQ, Mitchell P. Refractive errors in an older population: the Blue Mountains Eye Study. Ophthalmology 1999;106:1066-72.
French AN, Morgan IG, Burlutsky G, Mitchell P, Rose KA. Prevalence and 5- to 6-year incidence and progression of myopia and hyperopia in Australian schoolchildren. Ophthalmology 2013;120:1482-91.
McCullough SJ, O’Donoghue L, Saunders KJ. Six Year Refractive Change among White Children and Young Adults: Evidence for Significant Increase in Myopia among White Uk Children. PLoS One 2016;11:e0146332.
Bourne RR, Stevens GA, White RA, Smith JL, Flaxman SR, Price H, et al. Causes of vision loss worldwide, 1990-2010: a systematic analysis. The Lancet Global Health (Internet). 2013 13 November 2013.
Smith TST, Frick KD, Holden BA, Fricke TR, Naidoo KS, ‘Potential lost productivity resulting from the global burden of uncorrected refractive error’ in Bulletin of the World Health Organization, 2009; 87
Fricke, T. et al. Global cost of correcting vision impairment from uncorrected refractive error. Bulletin of the World Health Organization 90, 728-738 (2012).
Naidoo KS, Fricke TR, Frick KD, Jong M, Naduvilath TJ, Resnikoff S, Sankaridurg P. Potential Lost Productivity Resulting from the Global Burden of Myopia: Systematic Review, Meta-analysis, and Modeling. Ophthalmology. 2019 Mar;126(3):338-346. doi: 10.1016/j.ophtha.2018.10.029. Epub 2018 Oct 17. PMID: 30342076.
- Congdon N, Wang Y, Song Y, Choi K, Zhang M, Zhou Z, et al. Visual disability, visual function, and myopia among rural chinese secondary school children: the Xichang Pediatric Refractive Error Study (X-PRES)-report 1. Invest Ophthalmol Vis Sci. 2008;49(7):2888-94.).