Introduction
The recognition of myopia as a significant public health problem has driven the development and evaluation of numerous interventions to slow its progression and delay its onset, particularly since the International Myopia Institute’s 2019 review.1 This new 2025 article2 reviews the efficacy of such interventions. In summarizing the efficacy of mature technologies, only randomized controlled trials with a concurrent control group and axial length measures were included. An additional requirement was at least 12 months of follow-up. For newer and emerging treatments, the paper highlights both promise and the gaps that require further study.
Measuring Efficacy
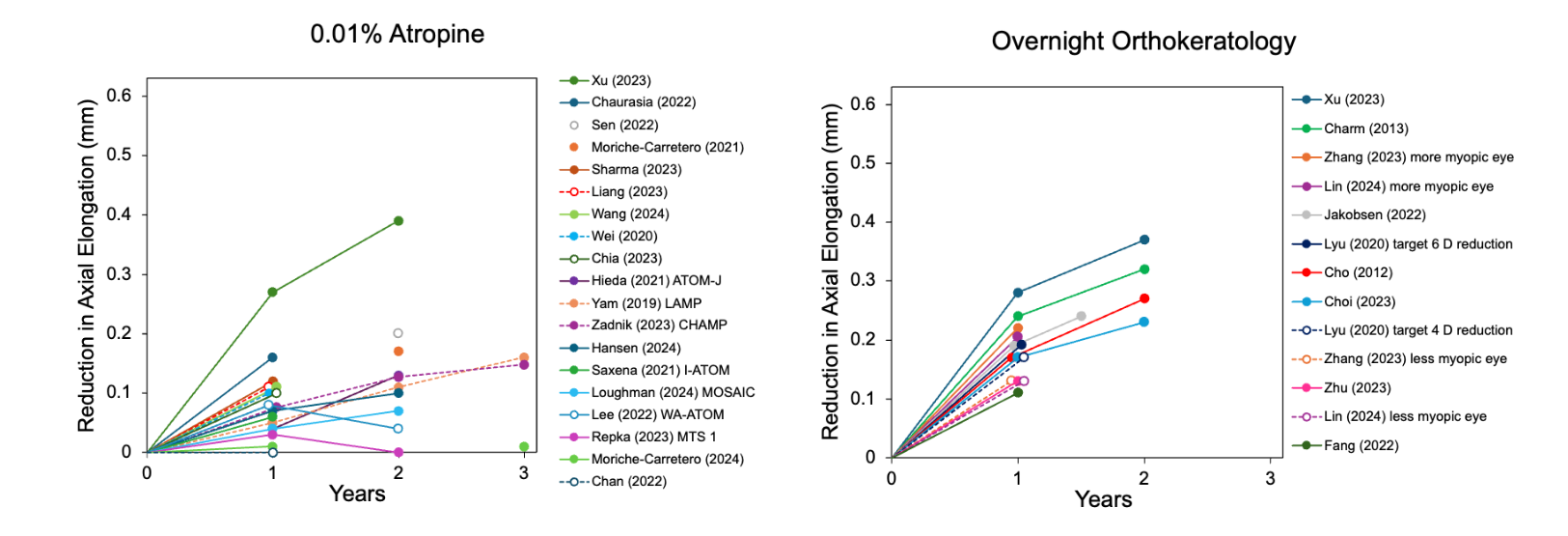
The efficacy of a myopia control intervention is described as slowing of axial elongation (in mm) or myopia progression (in D). Both are presented in the paper, although only axial elongation is shown graphically. Efficacy is time dependent, and the Figure below shows the relation between treatment efficacy (slowing of axial elongation) and study duration for six categories of interventions. Due to the heterogeneity in the study data, no meta-analyses were undertaken. Where treatments across different clinical trials were considered similar, e.g., orthokeratology, 0.01% atropine, and their combination, median (and interquartile range, IQR) were presented.
Efficacy of Myopia Control Modalities
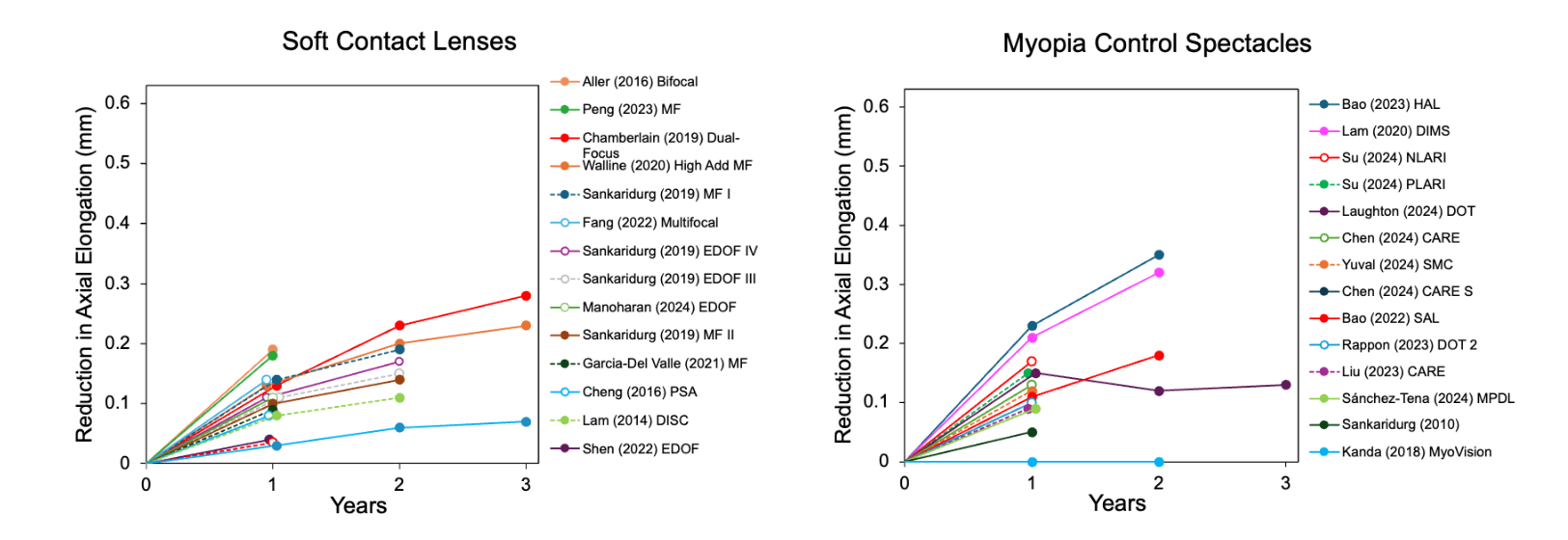
Spectacle Lenses: Recent advancements in lens designs for myopia control demonstrate significant potential. Ten randomized clinical trials were identified, with efficacy up to 0.35 mm over two years.
Soft Contact Lenses: Soft lenses with more than one focal power have been evaluated in 14 randomized clinical trials—12 with a concurrent control group and two using a contralateral eye design. The efficacy is up to 0.19 mm and 0.28 mm over one and three years, respectively.
Orthokeratology: Orthokeratology is among the most effective myopia control modalities with relatively consistent results across 10 randomized clinical trials. The median (IQR) one-year efficacy is 0.17 mm (0.13 to 0.20) and the median two-year efficacy is 0.30 mm (0.26 to 0.33).
Atropine: Clinical trials have consistently demonstrated atropine’s potential to slow myopia progression. There have been 21 randomized clinical trials of 0.01% atropine, all published since 2019. The median (IQR) one-year efficacy is 0.08 mm (0.05 to 0.12) and the median two-year efficacy is 0.12 mm (0.08 to 0.16). In addition, 9 randomized clinical trials have evaluated higher atropine concentrations with two-year efficacy up to 0.50 mm.
Combination Therapy: Combining optical and pharmacological treatments have the potential to offer additive or synergistic effects. To date, robust evidence is limited to 5 randomized clinical trials of combining overnight orthokeratology with 0.01% atropine. Two-year results show that efficacy is increased by a median of 0.12 mm by the addition of atropine to orthokeratology.
Light-Based Therapies: The evidence on how various characteristics of light may affect refractive development is reviewed comprehensively in a companion IMI paper.3 Ultraviolet light is relatively ineffective, while blue light stimulation of the optic nerve head is in the early stages of evaluation. The median (IQR) one-year efficacy of red-light therapy in 7 randomized clinical trials is 0.40 mm (0.38 to 0.42 mm), greater than any other treatment, and consistent across a range of devices. Nonetheless, there are safety concerns with decreases in foveal cone density documented and a report of a child experiencing bilateral vision loss after five months of red-light therapy.
Figure 1.

Interventions to Delay Myopia Onset
Earlier age of myopia onset is associated with higher myopia in adulthood; hence it is important to identify effective prophylactic interventions and implement them in children who are at risk of developing myopia. A number of randomized clinical trials of increased daily outdoor time have shown reductions in incident myopia (up to a 9% absolute reduction). Likewise, children receiving 0.05% atropine were half as likely to become myopic in a two-year randomized clinical trial as those on a placebo. Emerging evidence suggests the potential for optical methods to delay myopia onset.
Surgical Management of High Myopia
Surgical interventions for stabilizing the sclera have a long history, with interest revitalized by the increase in the prevalence of high myopia. In highly myopic children, posterior scleral reinforcement (PSR) has been evaluated, mainly in China. Among the 12 studies with a comparison group, the median (IQR) annual slowing of axial elongation is 0.19 mm (0.10 to 0.28). In adults, macular buckling (MB) may be applied to address existing pathological complications and visual impairment, and slow further deterioration in vision. Further research into safer and technically easier surgeries is warranted.
Conclusion
This comprehensive review illustrates the increase in myopia control clinical trials since previous IMI papers on the topic. Indeed, over 70% of the studies used to construct the Figure were published since 2020, demonstrating a massive proliferation of research on interventions to slow myopia progression. The Figure is unique in that it provides a comprehensive summary, demonstrating how efficacy varies within and across modalities, and as a function of treatment duration.
Summary
There are now multiple effective interventions available across most categories, giving clinicians real tools to manage myopia proactively.
No evidence of rebound was found for myopia control spectacles and soft contact lenses, echoing previous IMI statements. Conversely, five of the six highest rebound values (≥ 0.14 mm) were reported in studies of atropine or red-light therapy.
Although the primary focus of most clinical trials is efficacy, it is important to consider safety.
Withholding treatment from myopic children for long periods may no longer be considered ethical.
Understanding the mechanisms by which interventions could lead to more targeted and effective treatments.
References
1. Wildsoet CF, Chia A, Cho P, et al. IMI – Interventions Myopia Institute: Interventions for Controlling Myopia Onset and Progression Report. Invest Ophthalmol Vis Sci 2019;60(3):M106-M31. doi: 10.1167/iovs.18-25958
2. Bullimore MA, Saunders KJ, Baraas RC, et al. IMI-Interventions for Controlling Myopia Onset and Progression 2025. Invest Ophthalmol Vis Sci 2025;66(12):39. doi: 10.1167/iovs.66.12.39
3. Ashby R, Harb EN, Ostrin LA, et al. IMI—The Role of Light in Refractive Development and Myopia: Evidence from Animal and Human Studies. Investigative Ophthalmology & Visual Science 2025
Acknowledgments
This IMI White Paper was summarised by Prof. Mark A. Bullimore. A full list of the IMI taskforce members and the complete IMI white papers can be found at myopiainstitute.org. The publication and dissemination costs of the International Myopia Institute reports were supported by donations from the Brien Holden Vision Institute, Carl Zeiss Vision, CooperVision, EssilorLuxottica, Hoya, Thea, Alcon, and Oculus.
Citation
Mark A. Bullimore, Kathryn J. Saunders, Rigmor C. Baraas, David A. Berntsen, Zhi Chen, Audrey Wei Lin Chia, So Goto, Jun Jiang, Weizhong Lan, Nicola S. Logan, Raymond P. Najjar, Jan Roelof Polling, Scott A. Read, Emily C. Woodman-Pieterse, Noémi Széll, Pavan K. Verkicharla, Pei-Chang Wu, Xiaoying Zhu, James Loughman, Manbir Nagra, John R. Phillips, Huy D. M. Tran, Fuensanta A. Vera-Diaz, Jason Yam, Yue M. Liu, Sarah E. Singh, Christine F. Wildsoet; IMI—Interventions for Controlling Myopia Onset and Progression 2025. Invest. Ophthalmol. Vis. Sci. 2025;66(12):39 https://doi.org/10.1167/iovs.66.12.39.
Correspondence
Brien Holden Vision Institute Ltd
Level 4, North Wing, Rupert Myers Building, Gate 14 Barker Street,
University of New South Wales, UNSW NSW 2052
imi@bhvi.org